The solution to more effective cancer treatments may be closer to home than previously expected. The answer is not better chemotherapy or radiation, but cold. Cryoablation technology or the targeted use of extreme cold has previously been identified as treatment option for cancerous tumors and previously tested on invasive breast cancer carcinoma with promising results.
With more research and testing under its belt, cryoablation technology is now not only being tested to treat breast cancers and non malignant fibroadenomas, but also has been recently proven to treat patients with cancers of the kidney and prostate. Multiple studies supporting successful cryoablation treatment of kidney and prostate cancers was presented at the Society of International Radiology’s 34 Annual Scientific Meeting.
Cryoablation technology uses a catheter to selectively freeze the afflicting tumor and supplying vasculature without extensive damage to surrounding tissue or organs. A small cut in the skin can allow the probe to enter the affected area and freeze the tumor and supporting blood vessels. The procedure is significantly less invasive than normal surgery and is able to more precisely destroy harmful tissue while doing minimal damage to surrounding healthy tissue.

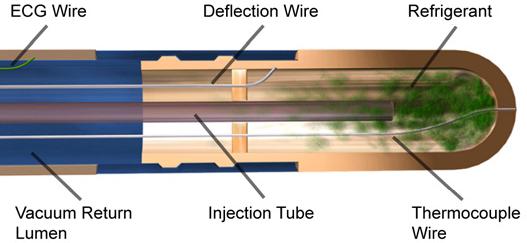
Photo: Pictorial representation of Cryoablation catheter, used in cryoablation therapy. Credit: Stanford Haptics
Patients undergoing cryoablation treatment are put under light anesthesia and a hollow needle is inserted through the skin directly into the tumor through help of an ultrasound and/or CT. The cryoprobe needle, filled with argon gas, reacts with the tumor and creates an ice ball, which quickly freezes the tumor. After two freezing and one thawing cycles, the tumor is frozen beyond its margin, ensuring the death of the whole tumor.
For patients with kidney cancer, cryoablation technology could easily mean the different between life and death. According to two studies presented at the Society of International Radiology’s 34 Annual Scientific Meeting, cryoablation could take center stage for primary action against kidney tumors. Kidney cancer affects more than 32,000 Americans each, may without any noticeable symptoms. More than 75 of cases are diagnosed when small tumors in the kidneys are discovered incidentally.
"Interventional cryoablation is as effective as laparoscopic surgery (partial nephrectomy), the current gold standard treatment … for treating renal cell carcinoma," said Christos Georgiades, M.D., Ph.D., interventional radiologist at Johns Hopkins Hospital in Baltimore, Md. "We can eliminate it … with a simple outpatient procedure. Eliminating cancer at such an early stage is truly significant news for kidney cancer patients."
According to the studies, conducted at John’s Hopkins University, the safety and efficacy of cryoablation was tested on percutaneous (no incision) methods, to demonstrate the abilities of the technology. Researchers looked at 90 tumors in 84 patients. Efficacy was determined based on a tumor's size at 3,6 and 12-month clinic visits and then yearly -- with follow-up imaging with CT or MRI scans. Both efficacy and three-year survival rates approach 100 percent overall. Results of the study showed that the ratio of patients whose renal cell carcinoma was completely destroyed by cryoablation was 100% for tumors measuring up to two inches, and nearly 100% for tumors up to three inches. Three larger four inch tumors were also treated and two of them were also successfully treated with cryoablation therapy.
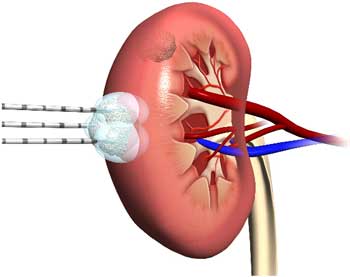
This illustration shows a kidney undergoing cryoablation therapy. Gaseous argon filled probes are inserted in the skin and inserted directly into the tumor. The freezing and thawing cycles ensure the death of the entire tumor by being pushed past its temperature edge. Picture credit: Westchester Medical Group
"Based on the results of our three-year study, we have shown that interventional cryoablation for kidney cancer should be the gold standard or the first treatment option for all patients whose tumors are 4 centimeters or smaller. It should be a viable option for patients whose cancer is even larger than that. And, ablation is a very effective option for patients who cannot or do not want to have surgery," noted Georgiades.
This success is good news for patients diagnosed with kidney cancer, who can opt for a minimally invasive and still effective cryoablation treatment, instead of surgically removing a large portion of their kidneys. Also promising is the success of cryoablation on tumors with larger mass, as the current notion is that the treatment only works on smaller tumors.
"Our studies highlight how effective interventional radiology treatments can be -- not just for kidney cancer -- but for other kinds of cancers and other diseases as well. Interventional radiology treatments will have a significant impact on the overall survival and benefits that patients can have from avoiding surgery," said Georgiades.
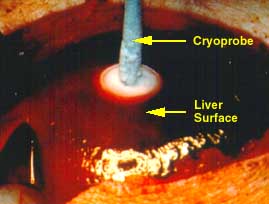
Photo:
Cyroablation technology used to treat liver cancer. "Ice-ball" is
visible where cryoprobe meets the tumor surface. Credit: University of Wisconsin, General Surgery
Supporting these claims for cryoablation technology are two additional studies also presented at the Society of Interventional Radiology’s 34 Annual Scientific Meeting which support results for effective cryoablation treatment for patients diagnosed with prostate cancer. 230,000 new cases of prostate cancer are diagnosed annually in the United States, with nearly 30,000 annual deaths.
Researches of the studies conclude from their data that focal cryoablation is just as effective for prostate cancer control as other treatment methods including surgery, radiation and hormone therapy, without the costs of trauma of invasive surgery, the risks of radiation and the other loss of sexual function caused by hormone treatments. Instead of removing the entire prostate, physicians can pinpoint exactly where invading tumors lie and tailor their cryoablation to treat the affected area.
For those diagnosed with prostate cancer, this means that removal of the entire prostate may not be necessary, if cryoablation therapy is possible.
"We've reached a tipping point: treating only the tumor instead of the whole prostate gland is a major and profound departure from the current thinking about prostate cancer," said study author Gary M. Onik, M.D., interventional radiologist and director of the Center for Safer Prostate Cancer Therapy in Orlando, Fla.
Since prostate cancer cannot be treated by “lumpectomy” or removal of the cancerous areas, cryoablation treatment is preferable considering that incontinence and erectile dysfunction that occur after surgery or other treatment can be avoided with the less invasive treatment.
"Any risks are fewer and lesser in intensity than surgery; so if you have the equivalent chance of cancer being cured with far less chance of having any complications, why wouldn't you choose it?" asks Onik.
Onik and colleagues studied 120 men who underwent cryoablation in the past 12 years. Of those patients, 93% had no evidence of further cancer, even with 72 patients having been labeled as “high-risk” for cancer reoccurrence.
"There were no local recurrences in the areas we treated, and with the ability to re-treat the 7 percent of patients who developed a focus of cancer at a different site in the gland; cryoablation was 100 percent effective in local control of the patient's disease," said Onik.
Just recently, the American Urological Association issued a best practice statement indicating that cryoablation treatment is an option for men with clinically-confirmed prostate cancer of any grade.
"There is no question that interventional cryoablation, which uses imaging to pinpoint tumors and probes to penetrate the skin to deliver freezing cold directly to a diseased tumor, works. This interventional treatment is not a widely known procedure yet, even to other doctors, and some patients are going to have to pursue it on their own," said Georgiades.
Cryoablation is approved by the Food and Drug Administration for treating soft tissue tumors, such as renal cell cancer, and other cancerous tumors.
References:
Abstract 18: "Percutaneous Cryoablation for Renal Cell Carcinoma: Safety," K. Hong, J. Geschwind, C. Georgiades, Johns Hopkins University--vascular and interventional radiology, Baltimore, Md.; R. Rodriguez, Johns Hopkins University--urology, Baltimore, Md.; and Z. Cizman, Jefferson University, Philadelphia, Pa., SIR 34th Annual Scientific Meeting March 7-12, 2009.
Abstract 19, "Percutaneous Cryoablation for Renal Cell Carcinoma: Efficacy," K. Hong, J. Geschwind, C. Georgiades, Johns Hopkins University--vascular and interventional radiology, Baltimore, Md.; R. Rodriguez, Johns Hopkins University--urology, Baltimore, Md.; and Z. Cizman, Johns Hopkins University--vascular and interventional radiology, Baltimore, Md., and Jefferson University, Philadelphia, Pa., SIR 34th Annual Scientific Meeting March 7-12, 2009.
Abstract 75: "Focal Therapy for Prostate Cancer -- 120 Patients With Up to 12-Year Follow-up," G. Onik, Center for Safer Prostate Cancer Therapy, Orlando, Fla., SIR 34th Annual Scientific Meeting March 7-12, 2009.
Abstract 198: "3D Prostate Mapping Biopsy Has a Potentially Significant Impact on Prostate Cancer Management," G. Onik, M. Miessau; Center for Safer Prostate Cancer Therapy, Orlando, Fla., SIR 34th Annual Scientific Meeting March 7-12, 2009.