Everyone
has heard about bisphenol
A
(BPA). It’s primarily used as a raw
material to make polycarbonate plastic and epoxy resins, both of which are high performance
materials used in many consumer products that help to make our
lives better and safer. But that’s
probably not what you’ve heard.
What
you may have heard is that we’re all exposed to BPA. And it’s true, we probably are all exposed to
BPA. But unless you’re an exposure
scientist who studies exposure to chemicals for a living, just knowing we’re
exposed to BPA isn’t very useful without knowing a lot more.
In
particular we need to know how much BPA we’re exposed to and whether those
levels are safe or not. That concept is
critical to understanding the safety of most anything we’re exposed to, whether
intentionally or not. For example,
taking one aspirin may safely eliminate your headache, but taking a whole
bottle of aspirin may eliminate your life.
The difference is important.
So
just how much BPA are we exposed to and are those levels safe? This is where an important new study
published in the journal Environmental
Pollution provides some very useful information. What the researchers realized is that an
enormous amount of data on consumer exposure to BPA is already available. It just wasn’t all in the same place where it
could be most useful, until now.
It’s
well known that people quickly eliminate BPA from the body through urine within
hours of exposure. Measuring BPA in
urine is considered the best way to evaluate exposure to BPA since what goes in
(i.e., exposure) comes out in urine where it’s easy to measure.
What
the researchers did was search the scientific literature for studies that
measured levels of BPA in urine. They
found more than just a few studies:
“[i]n total, we obtained over 140 peer-reviewed publications, which
contained over 85,000 data [points] for urinary BPA concentrations derived from
30 countries.”
The
researchers then sorted the data by age group (adult men and non-pregnant women,
pregnant women, and children) and country to assess whether exposure levels are
safe or unsafe for these groups. That
assessment was done by comparison of the exposure levels with safe intake
limits set by government bodies worldwide.
Compared
to what you may have heard, the results may surprise you: “[i]t is evident that the national and global
estimated human BPA daily intakes in this study are two to three orders of
magnitude lower than that of the TDI [Tolerable Daily Intake] … recommended by several countries.” In other words, actual exposure to BPA is
hundreds to thousands times below the safe intake limit.
These
results provide very strong support for the views of government bodies
worldwide on the safety of BPA. For
example, the U.S.
Food and Drug Administration (FDA) answers the
question “Is BPA safe?” with the unequivocal answer “Yes.”
What Did the Researchers Do and What
Did They Find?
As
noted by the researchers, “[t]o evaluate BPA’s potential risk to health, it is
important to know human daily intake.” In
general there are two ways to measure daily intake of a substance.
One
way is to measure how much of the substance goes into the body. A second way is to measure how much of the
substance comes out of the body as it is eliminated. The preferred approach for BPA, by far, is to
measure how much BPA is eliminated from the body in urine, a technique known as
urine biomonitoring.
The
reason is that BPA is efficiently converted in the body to a biologically
inactive metabolite after exposure, which is then quickly eliminated
from the body in urine. Essentially the
metabolite concentrates in urine, which makes it easy to measure with sensitive
analytical instruments. As noted
by a prominent group of researchers in regard to BPA and similar substances, “urine
is the most dependable biomonitoring matrix for population research.”
This
has not gone unnoticed by researchers who have generated urine biomonitoring
data on BPA for more than 10 years. What
the authors of this new study realized is that quite a bit of data has been
generated over this time period, but it is difficult to comprehensively
understand since the data is embedded in a wide variety of separate studies
that were conducted for different purposes.
To
resolve this dilemma, the authors searched the peer-reviewed scientific
literature for urine biomonitoring data on BPA regardless of why the data was
generated in the first place. By mining
the literature in this way, the authors uncovered an astounding amount of data
that, taken together, provides a deep understanding of human daily intake of
BPA.
Overall,
the authors found over 140 independent studies that reported urine
biomonitoring data for BPA. Together the
studies include more than 85,000 data points from individuals in 30
countries. The studies include a
significant amount of data for pregnant women and children, which is important
since these two groups are generally considered as subpopulations that might be
more sensitive to effects from chemical exposures.
What Does The Data Mean?
The
raw data that was analyzed simply measures the concentration of BPA, in the
form of its metabolite, in urine.
Without additional information, the raw data is difficult to understand
or interpret with respect to safety.
To
interpret the data, the researchers estimated daily intakes of BPA for
comparison with safe intake limits established by government bodies
worldwide. Intakes are fairly easy to
estimate since studies on human volunteers show that BPA is entirely eliminated
in urine after exposure. Essentially,
what goes in (i.e., intake of BPA) is equal to what comes out (i.e., amount of
the BPA metabolite in urine).
The
results were presented in an easy to understand graphical format as bar charts
that show estimated daily intakes of BPA by country for each of the three age
groups. For example, estimated intakes
for adults are shown in the bar chart below.
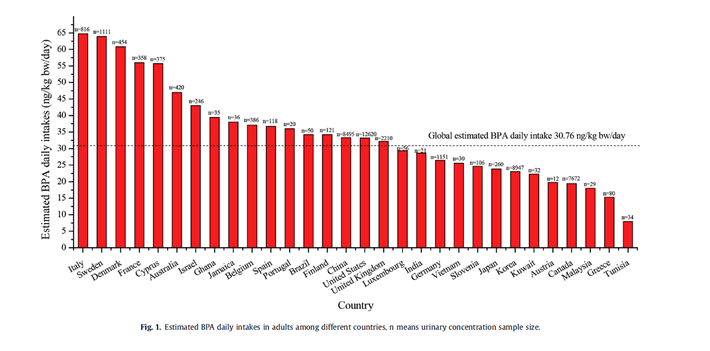
On
a global basis, the estimated daily intake of BPA for adults is approximately
31 nanograms BPA/kilogram bodyweight. Estimated
intakes on a country basis show only slight variation. With one exception on the low end, intakes
for all other countries range from approximately 20-60 nanograms/kilogram
bodyweight with each country differing from the global value by a factor of two
or less.
This
very low intake of BPA is consistent with how BPA is used and the low potential
for people to contact BPA. Most BPA is
chemically consumed as a raw material to make polycarbonate plastic and epoxy
resins. Although we contact these
materials in consumer products every day, the amount of residual BPA in these
materials is very low, typically less than 50 parts per million.
The
estimated daily intake for pregnant women is slightly higher at approximately
42 nanograms BPA/kilogram bodyweight and the estimated daily intake for
children is approximately 60 nanograms BPA/kilogram bodyweight. Since other studies have shown that most BPA
exposure comes from the diet, the relatively higher food intake for children
may account for the higher BPA intake.
The
authors also assessed whether their global daily intake estimates could be
considered to be representative of the global population. Based on other recent research and their own
analysis, the authors concluded that urine samples from a minimum of 1,000
people are required for an accurate estimate of daily intake for a
population.
Considering
the large amount of data available and analyzed in this study, the authors
noted that “the estimated global BPA daily intakes in this study for adults,
pregnant women and children were representative as the urine sample sizes were
over 16,000 [for each group]. To the
best of our knowledge, this is the first time that reasonable worldwide human
BPA daily intakes have been established for these population groups.”
Most
importantly, the authors concluded by comparing the estimated daily intakes of
BPA for each age group with the TDI (i.e., safe intake limit; 50 micrograms
BPA/kilogram bodyweight) for BPA that has been established in several
countries. In each case, as noted by the
authors, it is apparent that estimated daily intakes are two to three orders of
magnitude below the TDI. The TDI was
established to be protective of all age groups, including pregnant women and
children, so that conclusion is applicable to all age groups.
Since
estimated daily intakes varied only slightly by country, that conclusion is
also applicable to all countries. To go
back to where we started, is anyone safe from BPA? Based on a large amount of data the simple
answer is yes, we’re all safe from BPA.